Diabetic Eye Disease in Pregnancy
Diabetic Eye Disease in Pregnancy
In recognition of World Diabetes Day, Dr. R. A. Sharma, Secretary of The Ophthalmological Society shares his insights on Diabetic Eye Disease in Pregnancy
Diabetes is a condition where the body’s ability to use and store sugar is altered. This often results in too much sugar in the blood, which can cause damage throughout the body, including the eyes. Insulin is a hormone secreted by the body to control blood sugar levels. Diabetes can be classified in to Type 1 (in ability to produce insulin) and Type 2 (insulin resistance).
Diabetic retinopathy is a condition that occurs in people who have diabetes. It can cause progressive damage to the retina, which is the inside lining of the back of the eye that is responsible for vision. Diabetic retinopathy can be a serious sight-threatening complication of diabetes if left untreated.
Over the passage of time, diabetes damages the blood vessels in the retina. Diabetic retinopathy occurs when these tiny blood vessels leak blood, fluid and other materials. This results in damage to the retinal tissue manifesting itself as reduced vision. Both eyes are usually affected but may be asymmetrical. The longer a person has diabetes, the more likely they will develop diabetic retinopathy. However, the better the control of the blood sugar, the slower the onset and progression the retinopathy will be.
Symptoms of diabetic retinopathy include:
- Seeing floaters
- Blurred vision
- Having a dark or empty spot in the center of your vision
- Difficulty seeing well at night
When people with diabetes experience long periods of high blood sugar, fluid can accumulate in the lens inside the eye that controls focusing. This can change the curvature of the lens, leading to blurred vision. However, once blood sugar levels are controlled, the blurred vision should improve.
Often the early stages of diabetic retinopathy have no visual symptoms. This is because the changes in the eye may be occurring in the peripheral part of the retina (away from the centre part of the retina or visual axis). Early detection and treatment can reduce the potential for significant vision loss. This highlights the need for regular screening.
Treatment of diabetic retinopathy varies depending on the extent of the disease. People with diabetic retinopathy may need laser, injections into the eye, surgery or a combination of these to manage their stage of retinopathy. If you are diabetic, you can help prevent or slow the development of diabetic
Retinopathy by:
- Taking your prescribed medication
- Sticking to your diet
- Exercising regularly
- Controlling high blood pressure
- Avoiding alcohol and smoking
Pregnant women are at risk of developing diabetes during the pregnancy (Gestational Diabetes), or if diabetic already are at risk of suffering a worsening in their diabetic eye disease.
Diabetic retinopathy is not usually a significant complication in Gestational Diabetes, however, this is dependent on several factors and so these women do need regular screening from the discovery of diabetes to 12 months post delivery. In women with pre-existing diabetes, the exact cause of progression of the retinopathy is not fully understood but is thought to involve various processes:
1) Hormonal Changes: During pregnancy several hormones are produced in increased amounts. These include Oestrogen, Progesterone and Human Placental Lactogen. These cause changes in the blood vessel walls resulting in increased leakage from the vessels.
2) Circulatory Changes: During pregnancy, the blood volume and flow are increased. This results in increased leakage from the vessels that were already damaged by diabetes.
Those with Type 1 diabetes are more vulnerable to ocular changes in pregnancy.
Other risk factors include:
a) Duration of Diabetes
b) Severity of retinopathy before pregnancy
c) Level of diabetic control
d) Blood Pressure
These all contribute to a progression of retinopathy and may result in a reduction of vision. The treatment of diabetic retinopathy in pregnancy is very similar to that of non-pregnant diabetics described above. Subtle exceptions are the use of Injections into the eyes and surgery. This is because some of the medications injected are used to reduce the growth of new blood vessels in the eye and so control bleeding. However, the safety of these medications in pregnancy hasn’t been fully established as yet. As for surgery, often lying a heavily pregnant woman down for a long period of time to operate may not be comfortable for her.
As mentioned, screening for retinopathy/retinopathy progression is crucial in preventing vision loss. Screening should be done by an Ophthalmologist with a very low threshold for onward referral to a Retinal Specialist. In Gestational diabetes, the first screening should be done within 2 weeks of the diagnosis. Depending on the findings, repeat screening should be performed every 3-4 months until 12 months post delivery as a minimum. In pre-existing diabetes, frequently, these patients are being seen for screening already. However, where they are not, the first screening should coincide with the first antenatal clinic. Depending on findings, re-screening performed every 3 months until 12 months post delivery as a minimum. In many cases the diabetic retinopathy will show some regression after delivery. This in response to the reduction of exacerbating factors described above. However, it is worth remembering that vision loss will not reverse even if the retinopathy does after delivery. This underlines the importance of treating the progression of retinopathy as it occurs to prevent vision loss in the first place. It is
also worth noting that diabetic retinopathy is not a contraindication to Vaginal Delivery.
In summary, diabetes in pregnancy can have profound changes on the eyes and vision. Understanding this and screening for the changes will allow for treatment in a timely manner and so reduce the risk of vision loss.
Dr. R. A. Sharma is a practicing Ophthalmologist and Secretary of The Ophthalmological Society of the West Indies
READ MORETHE PATIENTS GUIDE TO KERATOCONUS
In recognition of World Keratoconus Day, Dr. Deo Singh of the Ophthalomogical Society of the West Indies
shares a patient’s guide to Keratoconus
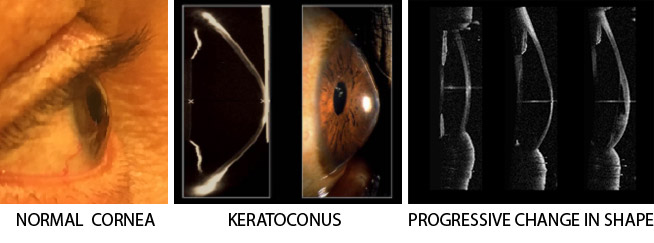
What is Keratoconus? A non-inflammatory condition in which the normally round front surface of the eye, the cornea, becomes increasingly steeper (more highly curved).
It results is stretching, thinning and irregularity of the cornea, increasing myopia (shortsightedness) and irregular astigmatism. Vision becomes increasingly blurred. Vision may initially be improved by spectacles but later contact lenses are required.
Severe cases appear like the tip of an ice cream cone i.e. conical. It may progress to scarring of the cornea requiring a corneal graft (transplant) operation to improve vision. KC often starts in the teens and progresses until the late twenties to thirties when it stabilizes or shows a reduction in the rate of progression.
HOW COMMON IS KERATOCONUS:
Keratoconus accounts for 60% of corneal transplants in Trinidad and Tobago.
CAUSATIVE FACTORS:
- Allergic conditions like Asthma*, Hay Fever, Sinusitis (The commonest associated factor in T&T is asthma.)
- Itchy Eyes and Eye Rubbing
SYMPTOMS:
- Blurred vision
- Distorted vision
- Needing to hold reading material close to the eyes
- Sensitivity to glare
- Multiple images or ghosting
- Frequent changes of spectacles or contact lenses
DIAGNOSIS
The diagnosis is suspected from:
- History of frequent changes in spectacle or contact lens prescription.
- Progressive blurring of vision.
- Increasing astigmatism.
- Itching and rubbing of the eyes.
- Family history of keratoconus.
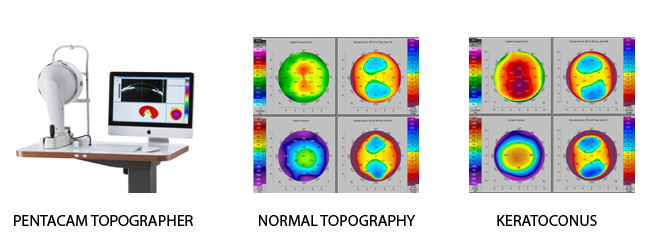
Corneal Topography
- This is a non-invasive method of mapping the curvatures of the corneal surfaces, assessing the degree of deviation from the normal cornea. Modern Topographers, like the Pentacam used, gives detailed a point-to point information of curvatures of the front and back surfaces and of the thickness of each point on the cornea.
- The cornea is normally responsible for two-thirds (2/3) of the focusing power of the Its topography is therefore very important to it’s function and the quality of vision.
MANAGEMENT:
- Allergy teatment
- Specific management of the individual patient depends on the severity and age of the patient.
- In early cases, spectacle or contact lens correction and monitoring by repeat Topography.
PREVENTIVE TREATMENT:
- Corneal Crosslinking Keratoconus – Introduced to Trinidad and Tobago at CEI 2008

CORNEAL CROSSLINKING is now considered the FIRST LINE of TREATMENT for KERATOCONUS.
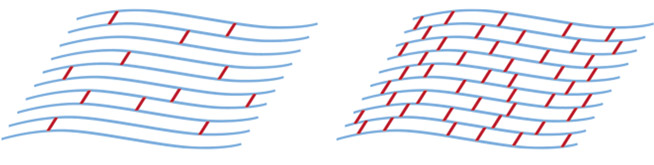
Ultraviolet corneal crosslinking (CxL) is the only treatment shown to slow the progression of keratoconus. It must be considered as the first line of treatment especially in young patients at diagnosis and before complications of the diaease or contact lenses occur. It reduces the need for corneal transplant surgery in keratoconus. CxL is a painless office procedure, under anaesthetic drops, not requiring injections, uses a special preparation of Riboflavin (Vit B2) drops and a low dose UV light. Treatment takes 45 mins to an hour.
It results in strengthening of the cornea that becomes more resistant to progressive deformation.
The figures show the parallel corneal layers and the collagen cross-linkages (red) which are increased after Cross Linking.
Strict criteria are used to determine the suitability of a given cornea for treatment. If the cornea has become too thin or scarred then crosslinking will be less useful and corneal transplant surgery will be needed.
Every young keratoconic patient must be referred to the Ophthalmologist for screening and for cornea crosslinking before being fitted with spectacles or contact lenses.
These lenses compensate for the focusing deficiency caused by the abnormality in corneal shape.
Spectacles and contact lenses DO NOT correct or treat the keratoconus and keratoconus often progresses (gets worse) in spite of contact lenses.
Contact lenses are often intolerable, do not fit properly, fall off the eye and do not give good vision as keratoconus gets worse. In more severe cases of keratoconus, contact lens wear may contribute to scarring of the cornea.
INTACS IMPLANTS are crescent shaped segments of similar material to intraocular lenses used in cataract surgery. They are implanted into the cornea in a procedure under local anaesthetic. They serve to reshape (flatten) the very steep cornea thereby improving vision. They also add structural stability.
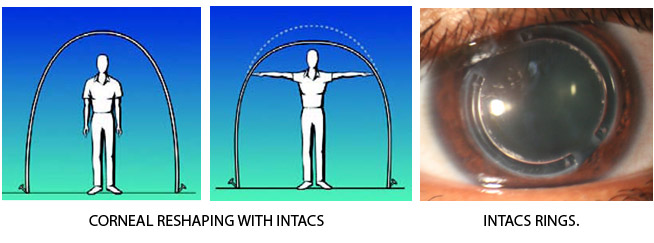
INTACS should not be used in keratoconus patients who can achieve functional vision on a daily basis using contact lenses, are younger than 21 years of age, do not have clear central corneas, and have a corneal thickness less than 450 μ at the proposed incision site.
CORNEAL TRANSPLANTS also known as corneal grafts or keratoplasties.
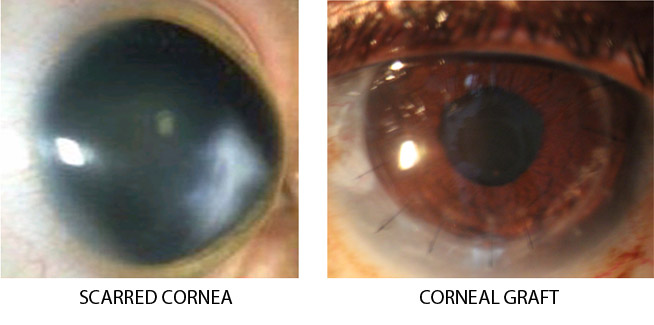
Full Thickness Corneal Transplant (also called Penetrating Keratoplasty – PK) is done when there is significant corneal scarring.
Partial Thickness Corneal Transplant surgery (Deep Anterior lamellar Keratoplasty – DALK) is done in earlier cases when it is not possible to get functionally comfortable vision with contact lens wear and there is only superficial scarring. DALK is an advanced form of
partial thickness corneal transplants that is specially suited for Keratoconic patients who do not have advanced scarring of the cornea because it protects against graft rejection and minimizes the need for a repeat graft in later years.
DALK advantages:
- Fewer problems with Rejection.
- Greater wound strength.
- Reduced regraft rate for young patients.
OSWI Celebrates World Keratoconus Day
PRESS RELEASE
OSWI Celebrates World Keratoconus Day
OSWI is pleased to join the rest of the world in celebrating World Keratoconus Day on November 10, 2017.
What is keratoconus?
The cornea is the clear window of the eye. It is responsible for refracting most of the light coming into the eye. Keratoconus blurs vision by thinning the cornea, the transparent front part of the eye. As the cornea thins, it begins to distort and bulge, and becomes cone-shaped rather than the usual round shape. Therefore, abnormalities of the cornea severely affect the way we see the world making simple tasks, like driving, watching TV or reading a book difficult. Significant loss of vision can result as the cornea is primarily responsible for the eye’s focusing power. Keratoconus is the most common corneal dystrophy in the US, affecting approximately one in every 2,000 Americans1 or approximately 170,000 people in the US. The Caribbean is no different as there are many people who have the disease and may not even be aware of it. The precise cause of keratoconus is unknown. It is thought that genetic factors may contribute, and that eye rubbing can lead to eye trauma, as well as trigger the release of enzymes which weaken the cornea. Eye rubbing can result from underlying diseases such as atopic or allergic conjunctivitis atopic or allergic conjunctivitis (swelling and inflammation of the whites of the eye, also known as pink eye).
Treatment Available in the Caribbean
Eyeglasses or soft contact lenses may be used to correct the mild nearsightedness and astigmatism caused in the early stages of keratoconus. As the disorder progresses and the cornea continues to thin and change shape, rigid gas permeable (RGP) contact lenses are generally prescribed to correct vision more adequately. The contact lenses must be carefully fitted, and frequent checkups and lens changes may be needed to achieve and maintain good vision. Intacs, intracorneal rings, are sometimes used to improve contact lens fit. Corneal crosslinking is also a new treatment option under investigation to halt the progression of keratoconus. In severe cases, a corneal transplant may be needed due to scarring, extreme thinning or contact lens intolerance. This is a surgical procedure that replaces the keratoconus cornea with healthy donor tissue. There are many treatments available right here in the Caribbean including crosslinking corneal surgery and intacs transplant
The Ophthalmological Society of the West Indies takes this opportunity on World Keratoconus Day to remind persons the importance of checking their eyes. If you are having problems with your eyes, you should visit your Ophthalmologist to get the necessary care and treatment.
READ MORETrinidad and Tobago Hosts World Sight Day Exhibition
In observance of World Sight Day, volunteers have partnered with the National Library and Information System Authority of Trinidad and Tobago (NALIS) to mount an eye care exhibition starting today and open until November 10 at the ground floor rotunda of the Port of Spain library.
The exhibition, which highlights eye health issues that impact lives everywhere, replaces the annual Walk For Sight organised since 2005 by the volunteers under the leadership of Dr. Desirée Murray, ophthalmologist and lecturer at The University of the West Indies, Del Philips, assistant professor, University of the Southern Caribbean, and Tayab Razac — medical representative Merck.
It will also honour this country’s first ophthalmic surgeon Dr Arthur Hutton McShine, mayor of Port of Spain from 1921-1922. He was a former student of Queen’s Royal College and served the Co-operative Bank for 32 years.
Specially invited guests will view the exhibition from 9.30 am on Wednesday after which the official opening ceremony will take place at 10am in the NALIS audiovisual room, corner Hart and Abercromby Streets. Anthony Smart, chairman of First Citizen’s Bank will deliver the feature address.

A symposium on eye care and blindness prevention, hosted by the University of the West Indies Faculty of Medical Sciences, Department of Clinical Surgical Sciences, will follow from 11.30am to 2pm. It is free and open to the public.
Topics to be discussed include cataract, glaucoma, pterygium, diabetic retinopathy, primary eye care, the red eye, uncorrected refractive error, prevention of falls in the elderly and prevention of eye injuries.
World Sight Day is an annual day of awareness which focuses global attention on blindness and vision impairment.
The 2017 call to action is Make Vision Count, with emphasis on those who are especially vulnerable: the young, school children and the elderly.
In Trinidad and Tobago, the major causes of avoidable blindness and vision impairment in these at risk groups include uncorrected refractive error, cataract, glaucoma and diabetes.

READ MORE
Eye care exhibition and UWI public symposium – 1st Nov 2017
In observance of World Sight Day, the Volunteers for World Sight Day is proud to partner with the National Library and Information System Authority of Trinidad and Tobago (NALIS) for an eye care exhibition which highlights eye health issues that impact lives everywhere. The eye care exhibition will also pay respects to the first Trinidadian ophthalmic surgeon, The Honourable Dr. Arthur Hutton McShine, who was Mayor of Port of Spain from 1921-1922. Dr. McShine, a former student of Queen’s Royal College, also served at the Co-operative Bank for 32 years, 28 of which he was President of the Board. The eye care exhibition will be located on the Ground Floor Rotunda of the Port of Spain Library and will run from Monday 30th October – Friday 10th November, 2017.
Specially invited guests will view the exhibition from 9:30 am on Wednesday 01st November, 2017, following which the official opening ceremony will take place from 10:00 am in the audiovisual room at NALIS , corner Hart and Abercromby Streets. Mr. Anthony Smart, Chairman, First Citizen’s Bank, will deliver the feature address. The official exhibition launch will be immediately followed by a public symposium on eye care and blindness prevention, hosted by the Department of Clinical Surgical Sciences, Faculty of Medical Sciences, The University of the West Indies.
World Sight Day is an annual day of awareness which focuses global attention on blindness and vision impairment. The 2017 call to action is “Make Vision Count”, with emphasis on those who are especially vulnerable: the young, school children and the elderly. In Trinidad and Tobago, the major causes of avoidable blindness and vision impairment in these at risk groups include uncorrected refractive error, cataract, glaucoma and diabetes. According the International Agency for the Prevention of Blindness, 253 million people are estimated to be visually impaired worldwide: 36 million are blind and 217 have low vision. About 89% of the world’s visually impaired live in low and middle-income countries. Eighty-two percent (82%) of people living with blindness are aged 50 and older, although this age group comprises only 20% of the world’s population. Eighty percent (80%) of all visual impairment can be prevented or cured. Here in Trinidad and Tobago, approximately 13,000 individuals are blind, with glaucoma (32%), cataract (29%) and diabetic retinopathy (13%) together accounting for 74% of blindness. Uncorrected refractive error accounts for 46% of moderate and severe visual impairment.
Since 2005, The Volunteers for World Sight Day, a non-profit, non-governmental organization based in Trinidad and Tobago, has worked to reverse these alarming statistics. Under the leadership of its chairperson, Dr. Desirée Murray, ophthalmologist and lecturer at The University of the West Indies, Ms. Del Philips, Assistant Professor, University of the Southern Caribbean, and Mr. Tayab Razac, medical representative Merck, this volunteer group coordinates meaningful events and activities which aid in the global effort to eliminate avoidable blindness. The Volunteers for World Sight Day was established to implement the agenda of the World Health Organization VISION 2020 initiative, by raising our nation’s awareness of healthy eye care practices through education and training initiatives, annual community events, collaboration with strategic partners and coordination with community groups in Trinidad and Tobago. This year, in lieu of the annual Walk for Sight, the volunteer group is proud to partner with the National Library and Information System Authority of Trinidad and Tobago (NALIS) for an eye care exhibition at the Port of Spain Library, corner Hart and Abercromby Streets, POS.
The exhibition places emphasis on the prevention of blindness (primary, secondary and tertiary prevention) and the rehabilitative services that are available for persons who are irreversibly blind. Representatives from PAVI (Persons Associated With Visual Impairment), the Caribbean Telecommunications Union, the Ministry of Health School Vision and Hearing Screening Programme and the Ministry of Social Development and Family Services, will be on site on Wednesday 1st November, 2017, to interact with the public and provide useful information. Commemorative bookmarks will be distributed.
In addition, the University of the West Indies Faculty of Medical Sciences, Department of Clinical Surgical Sciences, will host a public symposium on eye health and blindness prevention in the audiovisual room at the NALIS Port of Spain Library from 11:30 am – 3:00 pm on 1st November. Topics to be discussed include cataract, glaucoma, pterygium, diabetic retinopathy, primary eye care, the red eye, uncorrected refractive error, prevention of falls in the elderly and prevention of eye injuries. This symposium is free and open to the public.
Signed: Dr. Desirée Murray
On behalf of the Volunteers for World Sight Day team